
Better (UDS) Days Ahead

We all plan to do better next year. It’s an unofficial motto of anyone who reviews quality data. But, good intentions become reality with a solid plan. Any FQHC knows that by the time we submit the UDS report, it’s time to set in motion our plan to do better next year. The trick? How we decide which measure to focus on. In this post, we take a look at an example health center and recommend how we can maximize our HRSA QIA bonus as a way to set our priorities.
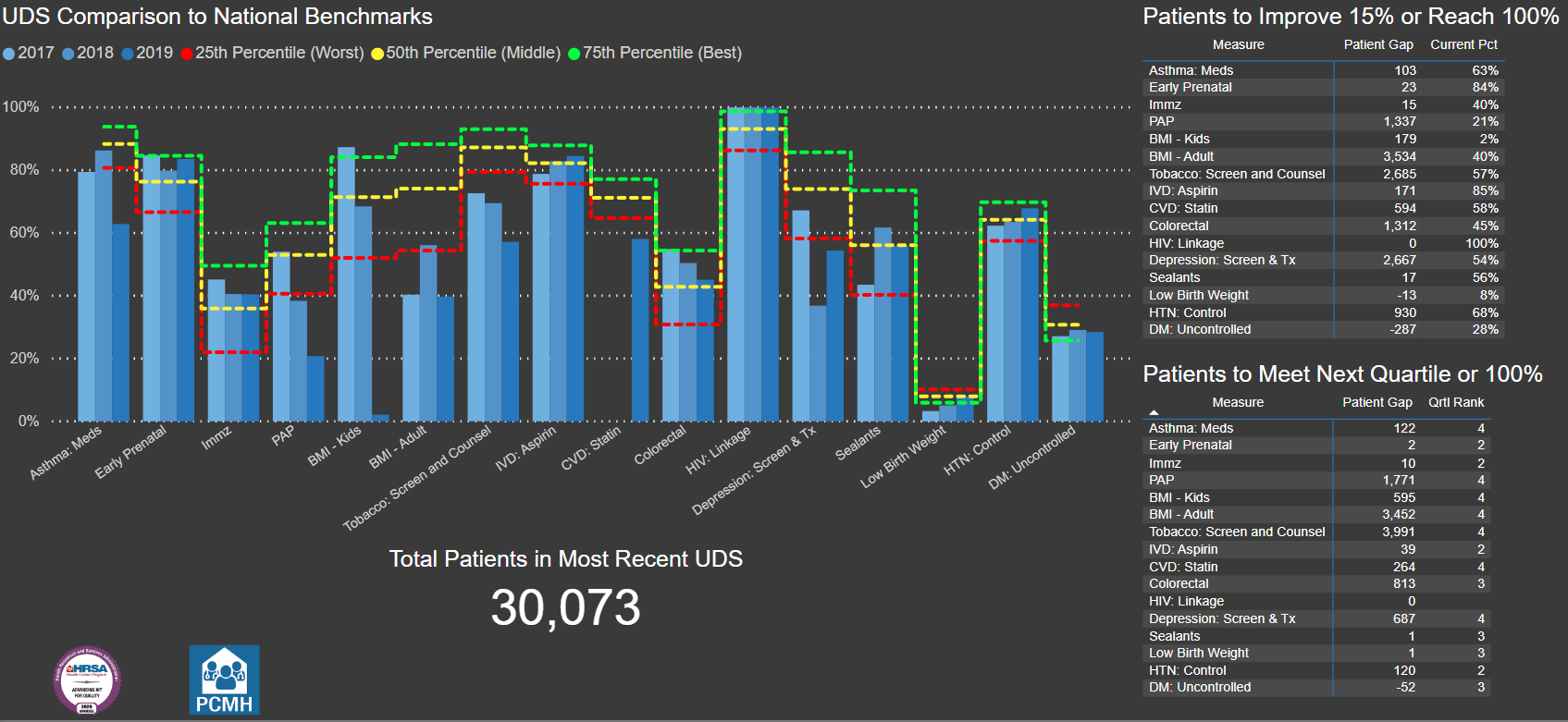
In the first post on HRSA Quality Improvement Awards (QIA), we outlined how the payments are calculated. In this post, we will look at a de-identified health center to discuss which measures should be a priority in order to maximize HRSA QIA dollars. The chart outlining the dependencies of the awards will be a helpful reference.
Let’s get started with our Microsoft PowerBI dashboard of the health center’s data.
What we Notice
Practice Size
The health center serves just at 30,000 patients a year across their service lines. This means they likely have around 15 to 20 providers, and may have 1 or 2 team members focused on quality, though they likely have other duties as well. In addition, it’s worth noting that this is a mid-sized health center that will require training and communication to implement any changes.
Awards
This health center is a Patient Center Medical Home (PCMH) and also received the Advancing HIT award. We know that the team for this health center has experience implementing EMR rules and creating policies that help track patient outcomes. In fact, the improvements we will identify can easily be turned into PDSA cycles for rapid improvement with focused attention.
Measure Details
Because this health center has already secured the PCMH and Advancing HIT awards, they must secure a Quality Award to win any additional funds. The Access Award, Value Award, and Health Disparities Reducer Award all depend directly or indirectly on receiving at least 1 quality award. Therefore, we need to review the measures to see which awards are easily eligible for 15% improvement or what it would take to meet the Health Center Leader or National Quality Leader awards.

In the table above, there are a few things we notice immediately:
Early Prenatal Access, Childhood Immunizations, Sealants, and Low Birth Weigh all have small numbers to advance 15%
The BMI for Kids is unusually low, and was a sharp drop off from previous years
Additionally, BMI for adults and Tobacco Screening have dropped from previous performance
Overall, the health center has relatively low scores for the quartile rank
We will discuss below which of the measures with smaller patient populations make sense to address. The BMI and Tobacco measures seem to combine nicely with a prevention screening and follow up interventions. Lastly, the low overall ranking scores suggest that the clinic should focus on the Clinical Improver Awards, and being to plan toward Health Center Leader Awards in subsequent years. To qualify for the Health Center Leader Award the average of the Adjusted Quartile Ranks needs to be 2.3 or lower for 2019 data.
Our Game Plan
Preventive Measures
First, this health center should devise a plan to review the clinic process and charting to address the Childhood Weight and Nutritional Counseling, Adult BMI and Follow Up, and Tobacco Screening and Cessation Counseling measures. The PDSA should follow these steps:
Review the report used to report these measures in 2020. Correct any missed CPTs or structured data the clinical team was using.
Run the data for these 3 measures with a rolling 12 months monthly to ensure a reliable reporting method.
Ensure that BMI and BMI Percentile are recorded on all patient visits. Especially BMI Percentile for pediatric visits, as this is sometimes omitted on sick visits.
Clarify the procedure codes, medications, or interventions that will meet the numerator criteria for each measure. Especially the Tobacco Cessation as different forms of verbal counselling, referrals to other professionals, or medications may meet this measure.
Conduct a quarterly sample chart review to validate the report data and correct any templates or charting that needs to be added to improve the performance.
Work with clinical leadership and IT to implement a clinical rule to add the Weight and Nutrition Counseling codes on Well Visits.
While the numerators are higher for these measures, once a systematic decision is made on how to capture these measures correctly, you may see a dramatic change as it is done for each visit.
Low Hanging Fruit
As for the measures with smaller patient panels, I would recommend for this practice to focus on the Dental Sealants and possibly the Early Prenatal Access.
The dental sealants should be considered because the dental team often has an ability to address quality measures because they have fewer measures than the medical team. Additionally, this measure is relatively easy to address as compared to other measures. A PDSA cycle can be set up to address:
Ensure all exclusion codes are correctly entered on the report (Caries conditions, Unerupted teeth, existing treatment, etc.)
Review current charts to ensure that these conditions are charted in the system in addition to planned treatment. Often the UDS reports will not exclude patients on planned treatment, but they will for conditions that meet the exclusion criteria.
Training for the team to chart conditions along with the treatment plan.
Training for the team to implement Caries Risk Assessments
Adjust the procedure to provide sealants same-day for any child coming in for comprehensive or periodic exam.
The Early Prenatal Access measure may be considered because it can be solved through close tracking and often leads to increased business for the practice by taking care of mom and then baby. This measure is admittedly harder, even though there are only 23 patients to make a difference over the previous year. A PDSA addressing the following items could be considered:
Ensure proper tracking in the EMR for when patients begin their prenatal care
Address the data gap for patients who did not start prenatal are with the health center but transferred in
Implement a positive pregnancy test tracking report and process to contact patients who do not have a scheduled prenatal visit and schedule their care
Clarify with clinical team and scheduling staff the health center’s protocols on which gestational ages will be seen for prenatal care, and the priority status for scheduling patients in their first trimester.
Conclusion
As this health center sets a focus on preventive screenings, dental sealants, and prenatal access, they set themselves up for Clinical Improver Awards in 5 categories. With focused attention, this health center should expect a $35,000 to $40,000 return on their investment. In many ways, this is what we should be doing. But, without an analysis like this, we can sometimes be left saying we need to focus on everything.
All of these measures are important, and we want to be the best at all of them. But we can’t always be the best at all of them right away.
Feel free to contact us to share your story of how you prioritize your measures, or schedule a review.